

Orserdu™ (elacestrant) is the first and only drug indicated for the treatment of ER-positive, HER2-negative, ESR1-mutated advanced or metastatic breast cancer in postmenopausal women or adult males whose disease has progressed after at least one line of endocrine therapy.
Unlike fulvestrant, which is the only approved selective oestrogen receptor degrader (SERD) for the indication and administered as an intramuscular injection, elacestrant is the first and the only oral SERD approved for the condition.
Recommended Buyers Guides
Initially developed by US-based biopharmaceutical company Radius Health, elacestrant became a part of the portfolio of Italian pharmaceutical and diagnostics company Menarini Group, following the in-licensing of the global development and commercialisation rights of the drug by the latter in July 2020.
Stemline Therapeutics, a wholly owned subsidiary of the Menarini Group, will commercialise the drug in the US.
Orserdu is available as a light blue, unscored, film-coated biconvex oral tablet in 345mg (oval) and 86mg (round) dosage strengths.
Regulatory approvals for Orserdu
The US Food and Drug Administration (FDA) granted fast-track designation to elacestrant in 2018.
In June 2022, Menarini and Radius Health submitted a new drug application (NDA) for elacestrant for the treatment of ER+/HER2- advanced or metastatic breast cancer to the FDA. The NDA was accepted under priority review in August 2022. The FDA approved Orserdu for the treatment of the condition in January 2023.
A marketing authorisation application (MAA) for Orserdu has also been submitted to the European Medicines Agency (EMA) and the same is currently under review.
Advanced or metastatic breast cancer causes and symptoms
Breast cancer is the second most common form of cancer that occurs in women. ESR1 mutations are seen in up to 40% of advanced or metastatic ER+, HER2-breast tumours. These mutations are a recognised cause of resistance to normal endocrine treatment, the cornerstone of treatment in metastatic hormone-driven breast cancers.
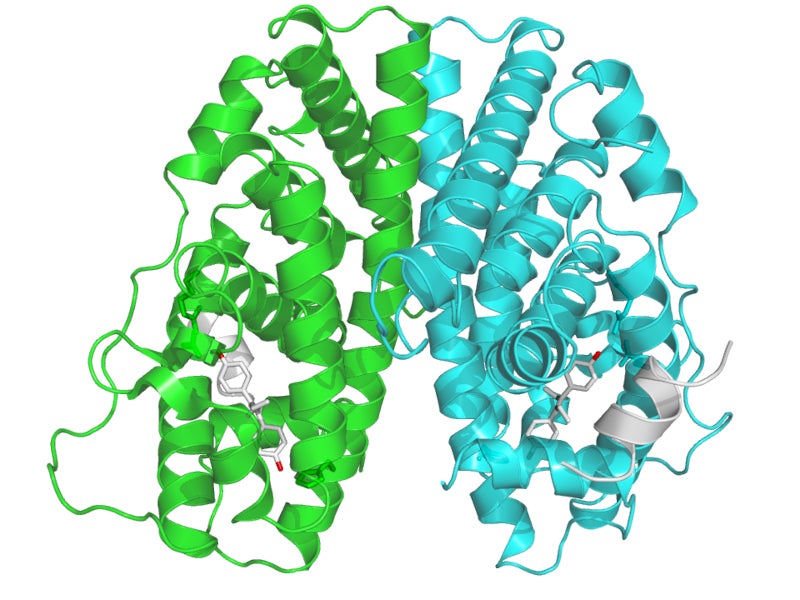
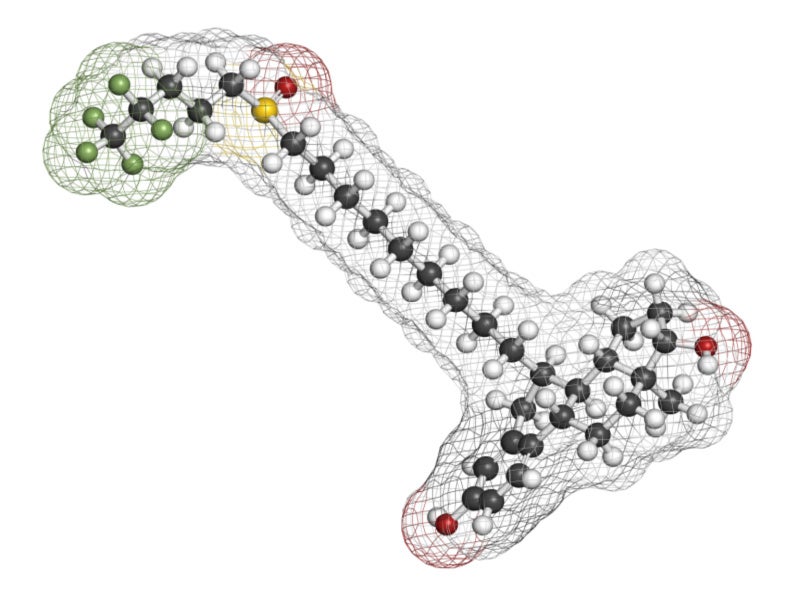
Elacestrant’s mechanism of action
Elacestrant is an oestrogen receptor antagonist that interacts with the oestrogen receptor-alpha (ERα) and inhibits 17-estradiol mediated cell growth in ER+, HER2- breast cancer cells at doses that triggered Erα protein degradation mediated through the proteasomal route.
Elacestrant showed anticancer activity in vitro and in vivo, including in ER+, HER2-breast cancer models resistant to fulvestrant and cyclin-dependent kinase 4/6 inhibitors, as well as those with ESR1 gene mutations.
Clinical trials on Orserdu
The FDA’s approval of Orserdu was based on a randomised, open-label, active-controlled, multi-centre, phase III clinical trial named EMERALD.
The drug’s efficacy was evaluated in 478 postmenopausal women and men with ER+/HER2-advanced or metastatic breast cancer, who had received one or more lines of endocrine therapy. Of the total patients recruited for the clinical trials, 228 had ESR1 mutations.
The patients were randomised in a 1:1 ratio to receive either Orserdu 345mg orally once daily or the investigator’s choice of endocrine treatment, which comprised either fulvestrant or an aromatase inhibitor (anastrozole, letrozole, or exemestane).
The primary efficacy outcome measures were progression-free survival (PFS) in the overall population and PFS in patients with tumours harbouring ESR1 mutations, determined by a blinded imaging review committee.
ESR1 mutational status was detected using blood-circulating tumour deoxyribonucleic acid (ctDNA) and was restricted to ESR1 missense mutations in the ligand binding region.
In the 228 patients with ESR1 mutations, the median PFS was 3.8 months in the elacestrant group and 1.9 months in the fulvestrant or aromatase inhibitor group.
An exploratory examination of PFS in the 52% of patients who did not have ESR1 mutations revealed a 0.86 hazard ratio (HR), indicating that the improvement found in the overall population was largely due to the outcomes reported in the subgroup of patients with an ESR1 mutation.
The trial demonstrated statistically significant PFS in patients with elacestrant versus standard-of-care endocrine monotherapy, satisfying both main objectives in all patients and those with ESR1 mutations.
The most common adverse reactions reported in patients treated with Orserdu were musculoskeletal pain, nausea, increased cholesterol, increased aspartate aminotransferase (AST), increased triglycerides, fatigue, decreased haemoglobin, vomiting, increased alanine aminotransferase (ALT), decreased sodium, increased creatinine, decreased appetite, diarrhoea, headache, constipation, abdominal pain, hot flush, and dyspepsia and laboratory abnormalities.