
Due to varied and evolving case definitions, the task of measuring dementia’s prevalence across time and borders has been hindered by heterogeneity. As a result, epidemiological indicators of its disease burden have required standardisation in order to allow for meaningful intergenerational and global comparison. In a novel study published in June 2025 in JAMA Open Network, Xiaoxue Dou and colleagues leveraged and standardised three large databases in Europe and the US to explore the prevalence of dementia across multiple geographies with distinct generational cohorts. The authors’ analysis shows that dementia prevalence, as well as the risk of developing dementia, is significantly lower in more recent birth cohorts across all studied geographic regions. GlobalData epidemiologists forecast that the diagnosed prevalent cases of dementia are expected to increase from over five million to nearly 5.9 million between 2025 and 2032 in the US and five major European markets (France, Germany, Italy, Spain, and the UK). Studies that allow for meaningful comparison of dementia indicators across countries and generational cohorts, such as that of Dou and colleagues, allow for a more nuanced study of dementia to guide clinical authorities and policymakers in their attempts to address the disease’s individual and social effects as its burden mounts over time.
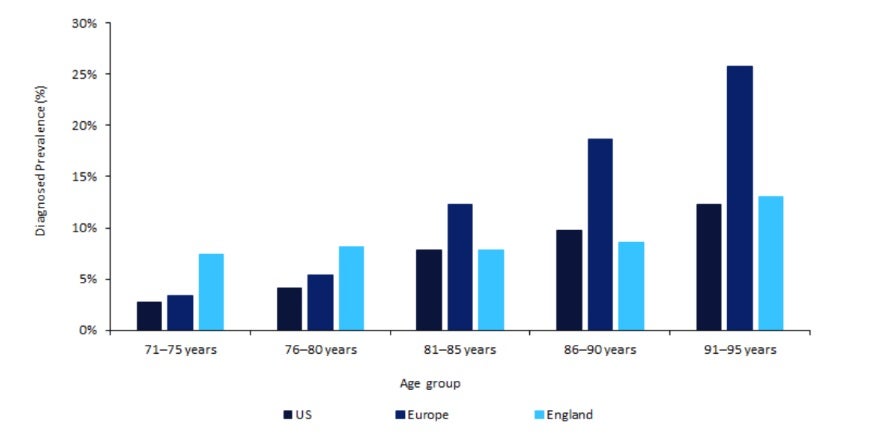
Dou and colleagues studied the prevalence of dementia across difference age cohorts in the US and Europe using three databases that measure health and aging in older adults: the US Health and Retirement Study, the UK’s English Longitudinal Study of Ageing, and Europe’s Survey of Health, Ageing, and Retirement in Europe (countries included are Austria, Germany, Sweden, the Netherlands, Spain, Italy, France, Denmark, Switzerland, and Belgium). Each dataset is nationally representative, and they were conducted between 1994 to 2021, 2002 to 2019, and 2004 to 2020, respectively, and in the aggregate capture 99,420 individuals aged 71 years or older. The authors segmented participants into four-year age groups from age 71 years to 96 years and over. To diagnose dementia in each cohort, the authors utilised a panel of experts whose diagnostic consensus was based on criteria in the third and fourth editions of the Diagnostic and Statistical Manual of Mental Disorders. As displayed in Figure 1, when comparing the frequency of dementia across the three regions, Dou and colleagues found that participants born more recently showed a lower diagnosed prevalence than that of older participants, suggesting a decline in the age-specific prevalence of dementia in all three geographies. The authors attribute this intergenerational heterogeneity to cohort-specific features and life experiences (eg, experiences with catastrophic events such as war, urbanisation, or varying levels of exposure to neurotoxic pollution).
Go deeper with GlobalData

Access deeper industry intelligence
Experience unmatched clarity with a single platform that combines unique data, AI, and human expertise.
In this large-scale study, Dou and colleagues present a compelling study design for cross-country comparisons of dementia prevalence in varying age cohorts. Moreover, they draw attention to important factors influencing the disease burden of dementia in different age groups, many of which are rooted in generation-specific environmental factors and life events. The novel methodology and findings from the authors present opportunities for further comparative research into dementia, as well as a case for policymaking and healthcare investment and practice in dementia care that acknowledges the nuance of intergenerational variation. As societies such as many of those in Europe and North America undergo demographic change to older populations on average, these considerations will be crucial in delivering on the needs of geriatric care.
