
Historical epidemiological analysis has demonstrated an association between urbanisation and growing cancer burden across the world due to factors such as increased ambient pollution and rising sedentism. In many countries in Latin America, urbanisation has occurred at a rapid pace, posing the risk for new public health concerns over a transition to environments that place residents at greater risk of cancer morbidity and mortality. In the first large-scale continental ecological study of cancer’s burden in Latin America’s metropolitan areas, Alfaro and colleagues have explored these emerging dynamics in a recent issue of The Lancet – Global Health. Their findings suggest a growing impact of cancers in the region’s cities, especially as a result of growing breast, colorectal, and lung cancer. In Mexico and Brazil, two of the major countries observed in the study, epidemiologists estimate the diagnosed incident cases of these three cancers will increase from nearly 346,000 to over 385,000 between 2025 and 2029. The growing burden of cancers in these and other urbanising Latin American countries poses a novel challenge for public health and clinical practitioners alike.
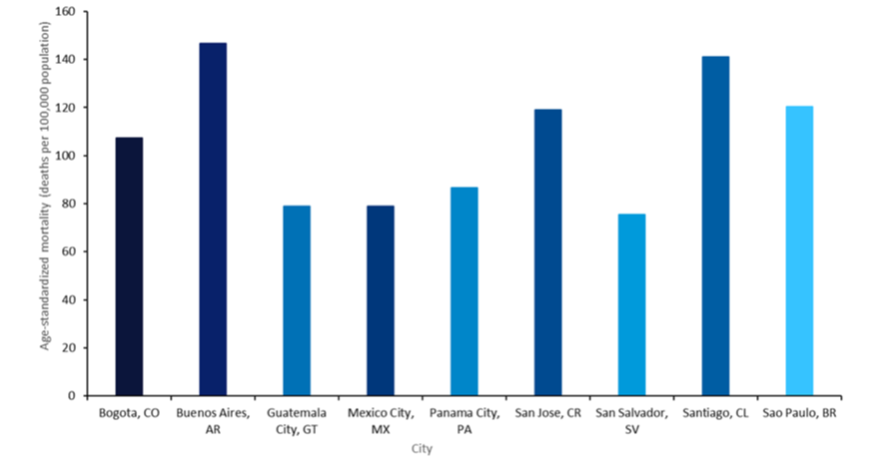
Alfaro and colleagues published their findings from analysis of the Salud Urbana en América Latina (SALURBAL) project, an expansive ecological study aimed at measuring cancer burden in 343 cities across Argentina, Brazil, Chile, Colombia, Costa Rica, El Salvador, Guatemala, Mexico, and Panama between 2015 and 2019. The authors defined ‘cities’ as any locale with at least 100,000 residents. Within these locales, the authors collected data on 1.5 million cancer deaths by way of International Classification of Disease codes focused on lung, stomach, colorectal, breast, and prostate cancer, due to their being the most common anatomical sites for cancers to occur. Cancer mortality was studied in tandem with measures of social-environmental and socioeconomic development in order to observe its relation to urbanisation. As displayed in Figure 1, the analysis suggested that cancer mortality across the continent’s cities is marked by high heterogeneity, with geography and sex being particularly determinative sources of variation. Among all measured cancers, cervical cancer was the most frequent among females while prostate was the most common among male patients. A last notable finding was that significant relationships were not observed between social-environmental development and cancer mortality. However, development did show a strong association with the frequency of certain cancer sites, with liver, stomach, cervical, and prostate cancer occurring more frequently in areas of lower development compared to colorectal and lung cancer in further developed urban environments.
The findings of Alfaro and colleagues present challenging takeaways that both defy and present opportunities for a coherent strategy in mitigating the impact of cancer on urban Latin America. Given the high heterogeneity of mortality across spatial, socioeconomic, and gender divides, a ‘one-size-fits-all’ approach to cancer’s management appears as unlikely as it would be ineffective. However, this shortcoming also builds a case for highly localised strategies for the surveillance, prevention, and treatment of cancer across the region. Given the hyperlocalised realities of cancer epidemiology in Latin America’s metropolitan areas, it is incumbent upon local authorities to embrace the parochial, devising strategies for the environments and inhabitants.
Go deeper with GlobalData

Access deeper industry intelligence
Experience unmatched clarity with a single platform that combines unique data, AI, and human expertise.
