Medical research has made great strides in understanding the diagnosis and management of Alzheimer’s disease (AD) and its related dementias (ADRD), but the bulk of this work has focused on its disease burden at late onset. Early-onset ADRD patients, defined as individuals experiencing the disease between 30 and 65 years of age, have undergone little investigation in spite of the disease’s growing prevalence.
Among the few emerging studies on early-onset ADRD is a recent publication by Xu and colleagues in the Journal of the American Medical Association (JAMA) comparing its distribution between rural and urban locales. While the authors found no significant relationship between rural or urban settings and increased prevalence of early-onset ADRD, they do note that rural residents experience lower diagnosis rates and higher reliance on primary care at the time of diagnosis. This has important implications for managing the disease due to the importance of a timely diagnosis in creating care plans. GlobalData epidemiologists expect a rise in AD cases across the 16 major pharmaceutical markets (16MM: US, France, Germany, Italy, Spain, UK, Japan, Australia, Brazil, Canada, China, India, Mexico, Russia, South Africa and South Korea), underscoring the importance of the equitable access to care in rural settings.
Go deeper with GlobalData

Access deeper industry intelligence
Experience unmatched clarity with a single platform that combines unique data, AI, and human expertise.
The authors reviewed more than 70,000 US commercial medical claims made between 2012 and 2017 for instances of early-onset ADRD. Positively diagnosed patients were segmented based on rural or urban residence, age and visits to primary care physicians (PCPs) or specialists. The analysis yielded nearly equal prevalence and incidence of early-onset ADRD between urban and rural settings. While locale showed no statistically significant impact on the disease’s basic epidemiology, it revealed disparities in care-seeking patterns.
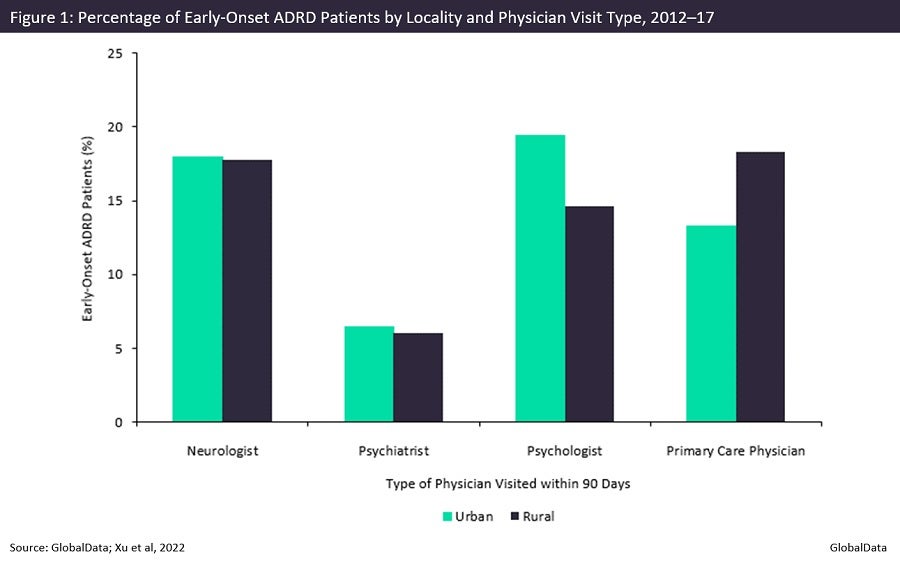
As seen in Figure 1, compared with the 13.27% of patients in urban environments, 18.32% of rural patients were more likely to rely on a PCP for an ADRD diagnosis. By contrast, only 14.60% visited a psychologist, significantly lower than the 19.42% of patients living in cities. The authors posit that the disparity in psychologist visits is related to the lower quantity of neuropsychological tests—integral pieces when diagnosing ADRD—administered to only 15.84% of rural patients. Despite the shortage of psychologist visits in rural settings, psychological tests were administered at a near-identical frequency. This contradiction suggests that rural PCPs may recruit the assistance of qualified health professionals such as social workers to perform psychological testing.
These findings captured the complex challenges and opportunities facing ADRD’s treatment and management in exurban locales. While individuals in urban settings are better positioned geographically to access relevant specialists, those in rural communities face a shortage of specialists within their vicinity. This presents them with the difficult choice of whether to forego specialist treatment or travel greater lengths to receive it. Reduced access to specialists qualified to administer neuropsychological testing potentially reduces or delays diagnosis, which is especially detrimental to early-onset ADRD patients given their propensity to multidomain cognitive impairments within a narrow window of disease onset.
The geographic disparities behind early-onset ADRD are symptomatic of a larger challenge in healthcare: bridging the urban-rural divide. Xu and colleagues propose leveraging the telecommunications boom caused by the outbreak of Covid-19. Using telemedicine platforms, rural patients may choose to consult specialists via virtual appointments. PCPs may, alternatively, rely on teleconferencing for direct access to specialists who can inform clinical decision-making. Although the technology is available, the authors identify the stigma surrounding psychological care and limited broadband access as the two most formidable hurdles that health professionals and policymakers have yet to fully resolve in rural communities.
GlobalData epidemiologists forecast that AD cases will rise from 11.7 million to nearly 16.1 million between 2018 and 2028. While forecasts do not include cases of AD aged younger than 60, its growing disease burden at all ages reinforces the need for research like the recent JAMA piece. The urban-rural divide in diagnosis patterns suggests that the current projections of ADRD may slightly undercount diagnosed prevalence. But if programmes such as those suggested in the piece are implemented within the coming years, this gap may be addressed near the end of the forecast period.